
While breast augmentation or mastopexy surgery performed separately have less potential risk and complications, breast augmentation/mastopexy surgery performed together carry a higher chance of complications and need for further surgery. For example, there is an increased risk of infection, implant exposure, breast asymmetry, loss of nipple-areola sensation, inability to breastfeed, mal-positioning of the nipple-areola complex, mal-position of the implants, wound healing problems, tissue necrosis, loss of blood supply to the nipple-areola complexes. Any of these complications may require further surgery, therefore, increasing the likelihood of revisionary surgery. To avoid these risks Dr. Pousti frequently recommends a ‘2-stage procedure’. The first stage is a breast lift followed by augmentation once the patient heals. Generally, good candidates for a 2-stage procedure are patients that need a significant amount of skin removed or patients interested in extra large implants.

Breast Implants Settling After Surgery
Before the procedure, the patient is examined by Dr. Pousti. The planned procedure of the first stage of the procedure (the mastopexy) is explained in detail.

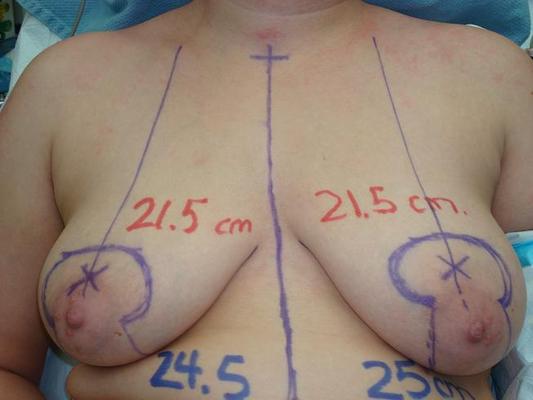


Once the patient is healed it is time for the second stage, the breast augmentation. Markings of the breast enhancement procedure are done before surgery as well.


The implants are placed in the breast pocket through a small incision. In most cases, Dr. Pousti will use the same incision site used for the breast lift to prevent further scarring.
Potential Risks and Complications
Breast augmentation/mastopexy (breast lifting) surgery is one of the most commonly requested breast contouring surgeries performed. Patients who seek to have this operation done generally wish to improve the contour of the breast by lifting the nipple-areola complex by tightening up the “skin envelope” and achieve increased fullness of the breasts especially superiorly and along the cleavage area. The combination breast augmentation/mastopexy surgery differs from breast augmentation surgery alone in that it carries increased risk compared to either breast augmentation or mastopexy surgery performed separately. Furthermore, the potential need for revisionary surgery is increased with breast augmentation/mastopexy surgery done at the same time. Revision mastopexy may also be necessary if the patient gains or loses weight or becomes pregnant. Loss of breast skin elasticity may contribute to the earlier need for revisionary surgery (repeat lifting) as well.
When breast augmentation/mastopexy surgery is performed, an implant is used below or on top of the pectoralis muscle. The breast tissue and skin are then elevated and lifted) to cover the breast implant. This “lifting” often involves skin excision, the areola, vertically and sometimes horizontally. This skin excision serves to tighten the “skin envelope”. By doing so, a lifted appearance of the breast is achieved and the loose-saggy appearance and feel of breast tissue is eliminated. Herein lies the competition and the potential risks and complications: the mastopexy procedure by definition involves reducing the skin envelope allowing for repositioning of the nipple-areola (and reshaping the breast). Breast augmentation by definition enlarges the breast and expands the skin envelope. Also, the placement of an implant necessitates the dissection of a “pocket” that reduces blood flow. The blood flow is further compromised by incisions used to reduce the skin envelope. Because of these factors, while breast augmentation OR mastopexy surgery is relatively simple and complication-free, breast augmentation/mastopexy surgery done together carries increased chances of complications and the need for further surgery. For example, there is an increased risk of infection, implant exposure, breast asymmetry, loss of nipple-areola sensation, inability to breastfeed, mal-positioning of the nipple-areola complex, mal-position of the implants, wound healing problems, tissue necrosis, loss of blood supply to the nipple-areola complexes. Any of these complications may require further surgery, therefore, increasing the likelihood of revisionary surgery. The patient must understand the principles behind any planned procedure of breast augmentation/mastopexy surgery. An understanding of the procedure will facilitate an understanding of the potential risks and complications when they occur. A well-informed patient may decide to stage the procedures (for example, perform the breast lifting operation initially followed by breast augmentation at a later date). A well-informed patient who decides to proceed with single stage breast augmentation/mastopexy procedure should understand the nature of the procedure, the increased potential risks, and complications so the combined procedures (compared to the procedures performed individually), and the higher likelihood of revisionary surgery to correct imperfections that arise from the combined procedures. This revisionary surgery may impose additional discomfort, recovery time, time off of work, and cost to the patient. To summarize, single-staged breast augmentation/mastopexy surgery carries increased risk compared to either of the procedures done separately. For the patient to make a well-informed decision, she must understand the potential increased risks and complications as well as the potential need for further surgery when the single staged procedure is performed. This will allow the patient an opportunity to proceed with two staged procedures (procedures done separately) or proceed with the single staged procedure with the increased risk of potential risk and complications and need for further surgery
Example of a 2-staged Surgery

Once healed, the patient can proceed with the second stage of surgery.


What To Expect After Surgery
Pain is rarely strong, more commonly being a degree of discomfort. Swelling occurs but usually begins to subside by the third or fourth day. Some degree of swelling may persist for longer periods. A well-fitted bra is worn day and night for four weeks. While there is probably seldom interference with future breastfeeding, women are cautioned that it may not be possible to breastfeed in the future. Driving may be resumed in 2 weeks. Non-contact sports in 3 weeks. Contact sports in 6 weeks. Sexual activity in 2 weeks.
